The second half of a two part series on oxygen toxicity, first published in Diver Magazine in Feb/Mar 2009. Last column we focused mainly on the mechanisms of oxygen toxicity.
This column will continue that discussion with a description of the toxic effects of oxygen on the lungs and the brain. The discussion is fairly technical so it would be advisable to review the last column before continuing with this one.
Dr. J. Lorrain Smith first described the toxic effect of oxygen on the lungs in 1899. He noted that the severity of the effect increased with increasing pO2 and that the effects where largely reversible. As shown in the diagram, the toxic effects of oxygen at partial pressures between 0.45 ATA and 1.6 ATA are primarily on the lungs while the toxic effect at pO2s over 1.6 ATA are primarily on the brain.
The earliest sign of pulmonary (lung) oxygen toxicity is a mild irritation in the trachea (throat) that is made worse with deep inspiration. A mild cough develops next, followed by more severe irritation and cough until inspiration becomes quite painful and the cough becomes uncontrollable. If exposure to oxygen is continued, the person will notice chest tightness, difficulty breathing, shortness of breath, and if exposure is continued long enough, the person will die, from lack of oxygen! The progressive damage to the lungs eventually makes it impossible for the oxygen to get to the blood as it passes through the lungs.

The time to onset of symptoms is highly variable but most individuals can tolerate 12-16 hours of oxygen at 1.0 ATA, 8-14 hours at 1.5 ATA, and 3-6 hours at 2.0 ATA before developing mild symptoms. There are several ways to track developing pulmonary oxygen toxicity but the most sensitive and accurate is the development of symptoms. A second technique is to monitor the vital capacity. Vital capacity (the amount of air that can be moved in one large breath) decreases with increasing pulmonary toxicity. A reduction of approximately 2% in vital capacity correlates with mild symptoms while a reduction of 10% correlates symptoms so severe that most individuals will not voluntarily continue breathing oxygen. These mild effects are completely reversible and no permanent lung damage occurs. However, the damage will take 2 to 4 weeks to heal. The pathology of pulmonary oxygen toxicity is understood but beyond the scope of this discussion.
A third way to keep track, in rough terms, of pulmonary oxygen toxicity is to keep track of the oxygen exposure. This technique is called calculating the Unit Pulmonary Toxic Dose (UPTD) and one UPTD is equivalent to breathing 100% oxygen, for one minute, at 1.0 ATA. As a guide, 615 UPTDs in one day will cause a 2% reduction in vital capacity and 1,425 units will cause a 10% decrease. There are several different ways to calculate the UPTD (some try to correct for increasing toxic effects with increasing dose, in addition to the simple pO2) and there is quite wide variation in individual tolerance so that symptoms are still the best guide. The situation where UPTDs are most useful is in planning a large number of dives, in a few days, all involving a large amount of oxygen decompression or CCR diving. Even then, the dive plan may have to be altered if the diver develops symptoms of pulmonary toxicity.
The first and most important method to prevent pulmonary oxygen toxicity is to limit exposure to the lowest possible pO2 for the shortest period of time. If you dive only air and limit your depth to a maximum of 130 fsw (40 msw), pulmonary oxygen toxicity is unlikely to be a problem. The second method to prevent pulmonary oxygen toxicity is to provide air breaks. The damage to the cells is cumulative and if for every 25 minutes of oxygen exposure you provide the cells with a five-minute period where the diver breathes air, the diver can tolerate twice as much oxygen before toxic symptoms develop when air breaks are given compared to breathing oxygen continuously. Basically what happens is that during the air breaks the cells are repairing the damage due to O2 radicals much faster than damage is occurring so they ‘catch up’ on some of the damage. Therefore, it will take much longer for a given level of damage to accumulate.
Oxygen toxicity of the brain (CNS) is a problem of higher pO2s for shorter periods of time. While breathing air, a pO2 of 1.6 ATA is not reached until a depth of 218 fsw (67 msw). Therefore, CNS oxygen toxicity is not a problem for standard recreational diving. However, more and more divers are using Nitrox and if you dive breathing a 40% oxygen mixture, the pO2 will be 1.6 ATA at a depth of only 99 fsw (30 msw) and if you decompress on 100% oxygen, the pO2 will be 1.6 ATA at a depth of 20 fsw (6 msw)! Therefore, CNS oxygen toxicity is a serious problem for some recreational divers, and a major problem for technical and commercial divers.
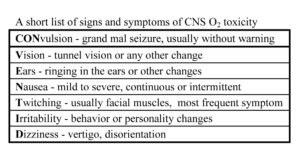
The first and most serious sign of CNS oxygen toxicity is often a grand-mal type convulsion. There are many other signs and symptoms of oxygen toxicity but there is no consistent warning that a seizure is about to occur. Even the EEG is completely normal until the convulsion starts. The convulsion due to oxygen toxicity is not believed to cause any permanent problems in and of itself because the body starts the convulsion with a surplus of oxygen on board and thus the hypoxia seen with normal seizures does not occur. However, the diver who convulses while in the water may drown or, if they ascend while the glottis is closed, may suffer pulmonary barotrauma.
There is huge variation in the amount of oxygen individuals can tolerate before they show signs of CNS oxygen toxicity and of even more concern, a huge variation in the same person on different days. A diver may do many dives in which they are exposed to high pO2s with no difficulties and falsely conclude that they are resistant to oxygen toxicity. Then, for no apparent reason, they may suffer a CNS hit on a dive where they are exposed to a lower pO2. In general, people can tolerate more oxygen in a dry chamber than in the water. In fact, most divers can tolerate two hours of oxygen at 3.0 ATA (66 fsw or 20 msw) in a chamber with few difficulties. While exercising in the water however, several divers have had convulsions at pO2s as low as 1.6 ATA. To make matters worse, in the chamber divers often have one of the less serious signs of oxygen toxicity such as tunnel vision, ringing in the ears or twitching, whereas in the water the first sign is often a seizure. The seizure starts with an immediate loss of consciousness and a period of about 30 seconds when the muscles are relaxed. All of the muscles of the body then contract violently for about one minute. The diver then begins to breathe rapidly and is very confused for several minutes afterwards. As you can well imagine, if this happens during a dive, the diver usually dies. The table gives a short list of the signs and symptoms of CNS oxygen toxicity but almost anything is possible.
There are some factors that are known to increase the risk of CNS oxygen toxicity. I have already mentioned two, submersion in water and working hard. The risk with working hard is that the pCO2 in the body is increased and this increases the blood flow to the brain. Other causes of increased pCO2 are skip breathing and increased carbon dioxide in the breathing gas. Increased stress on the diver and increased levels of adrenaline, atropine, aspirin, amphetamine and other stimulants all seem to increase the risk of CNS oxygen toxicity.

There are no drugs that can be used to prevent CNS oxygen toxicity. In animal experiments, the seizures could be prevented but the CNS cellular damage found after prolonged seizures still occurred. The only effective methods to prevent CNS oxygen toxicity are to limit the pO2, the time of exposure, and to give air breaks during oxygen breathing.
As general guidelines, the pO2 during decompression while at rest should never exceed 2.0 ATA and most divers use 100% oxygen at a maximum depth of 20 fsw (6 msw, 1.6 ATA). During the active part of the dive, the pO2 should never exceed 1.6 ATA and many divers are using 1.5, 1.4, or even 1.3 as the maximum pO2 for all parts of the dive. NOAA, the US Navy, the Royal Navy, the Canadian Forces, and many other organizations have guidelines for acceptable pO2s and the maximum time that may be spent at each. If you are interested in diving where you will be exposed to increased pO2, it is imperative that you get appropriate training.










